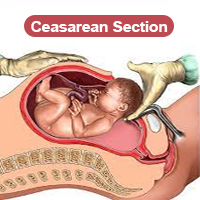
A lower (uterine) segment Caesarean section (LSCS) is the most commonly used type of Caesarean section used today. It includes a transverse cut just above the edge of thebladder and results in less blood loss and is easier to repair than other types of Caesarean sections.
It may be transverse (the usual) or vertical in the following conditions
The location of an LSCS is beneficial for the following reasons:
Most bleeding takes place from the angles of the incision, and forceps can be applied to control it.
Indications for caesarean section include fetal distress, cephalopelvic disproportion, failure of labour to progress, previous caesarean section (check what the indications were for this), placenta praevia, malpresentation and malposition, and prolapse of the cord. Caesarean section may also be indicated in cases of soft-tissue obstruction or scarring, diabetes, poor obstetric history, toxaemia, abruptio placentae, placental insufficiency, Rh incompatibility, and failed induction, and in older primigravidae.
Assessment
Examine the patient for pallor, oedema, abnormal blood pressure, and heart and lung disease and take appropriate action. Determine the fetal lie and presentation, and check for the presence of fetal heart sounds. For elective caesarean section, a vaginal examination is generally omitted; in emergencies the need will vary.
Investigations
Measure the patient’s haemoglobin level and test the urine for sugar and protein. Send a sample of blood for grouping (including Rh factor) and cross-matching. Test for bleeding and clotting times and for syphilis. If diabetes is suspected, include a test for fasting postprandial blood sugar.
Preoperative management
Perform the elective operation about a week before the expected date of delivery. Admit the patient the day before the operation and give a soap and water enema on the morning of the operation. Patients in labour should be given an antacid every 2 hours to neutralize gastric acid and so minimize the effects of any accidental aspiration of gastric fluid. An intravenous drip should be set up.
Equipment
See tray for Caesarean section, Annex 1.
Technique
The recommended procedure is transperitoneal, lower-segment caesarean section with a transverse incision into the uterus.
Empty the patient’s bladder by catheterization and then tilt her to her left by placing a pillow under her lower back on the right. A general or regional anaesthetic should be given. Prepare and drape the abdomen. Make a midline sub-umbilical incision (Fig. 2.3A). Incise the loose peritoneum covering the anterior surface of the lower uterine segment and push it downwards with the bladder (Fig. 2.3B). Make a small, transverse incision in the lower segment of the uterus crossing the midline 2 cm below the site of peritoneal incision. Widen the incision bluntly on either side (Fig. 2.3C). Rupture the membranes if they are still intact.
The aim is to deliver the baby as quickly as possible. For head-presentation delivery, carefully insinuate your fingers between the lower uterine flap and the head and hook them round the head (Fig. 2.3D). If the head is deeply engaged and difficult to extract, ask an assistant to dislodge it from the vagina (with gloved hands). A single forceps blade may be required to deliver it. In breech presentation, deliver the arms and the head carefully so as not to enlarge the uterine wound unduly. In cases of transverse lie, deliver the breech first after internal podalic version. An undiagnosed constriction ring may prevent delivery of the head; in such cases the ring must be cut vertically in the course of caesarean section, although this can result in a weak scar (ideally, this condition will have been suspected beforehand).
Fig. 2.3. Lower-segment caesarean section. Site of midline subumbilical incision (A); incising and pushing down the loose peritoneal covering of the anterior surface of the uterus (B); widening the incision into the uterus (C); hooking the baby’s head with the fingers (D); inserting the first layer of suture (muscle layer) (E). Inserting the second layer of suture, taking the muscles and burying the first layer (F); inserting the peritoneal layer of suture (G).
Extract the fetus. Clean and aspirate fluids from the nose and mouth. Divide the cord between clamps and ligate it. Give the mother 0.25 mg of ergometrine intravenously, and then remove the placenta and membranes. Rub the uterus if it is flabby, and, if necessary, start the patient on a drip of 4 or 8 IU of oxytocin (the amount to be determined according to the patient’s response) in 500 ml of 5% (50 g/litre) glucose at a rare of 15 drops/min.
Grasp the edges of the uterine incision with haemostatic (Green-Armytage) forceps. Stitch the incision in three layers. First insert a continuous, muscle-layer stitch of No. 1 chromic catgut on a half-circle, round-bodied needle; avoid the decidua and take the angles carefully (Fig. 2.3E). Then take up any unstitched muscle tissue and bury the inner layer of suture (Fig. 2.3F). Finally, close the visceral peritoneum with 0 chromic catgut (Fig. 2.3G). Complete abdominal toilet and close the abdominal wall in layers. Apply a sterile dressing.
Complications
Possible complications include primary haemorrhage that can lead to hypovolaemic shock, sepsis with peritonitis, secondary haemorrhage, retrovesical haematoma formation, and pulmonary embolism

Dr. Vikas Chhabra is Specialist in General Surgery & have 22 Yrs Experience in General, Laproscopic, Endourology, Plastic & Laser Surgeries.

Dr. Kiran Chhabra is famous Consultant of IVF, She is Specialist in Gynaecology & practicing Gynae, Obs & Infertility since 2003.

Dr. Aman Chhabra is famous Orthopedic Surgeon, He is Specialist in Ortho, Hand Surgery & Joint Replacement and have more than 15 Yrs Experience.
View More
Test Tube Baby Centre
Operation Theatre
Ventilator
ICU
OPD
Ultrasound
Colour Doppler
Laboratory
Patient Rooms
Pharmacy
24 Hours Service
Chhabra Hospital &
Test Tube Baby Centre
Near Stadium,
80 Feet Road,
Bathinda (Punjab)
Pin: 151001